What is POTS? Understanding Postural Orthostatic Tachycardia Syndrome
Introduction
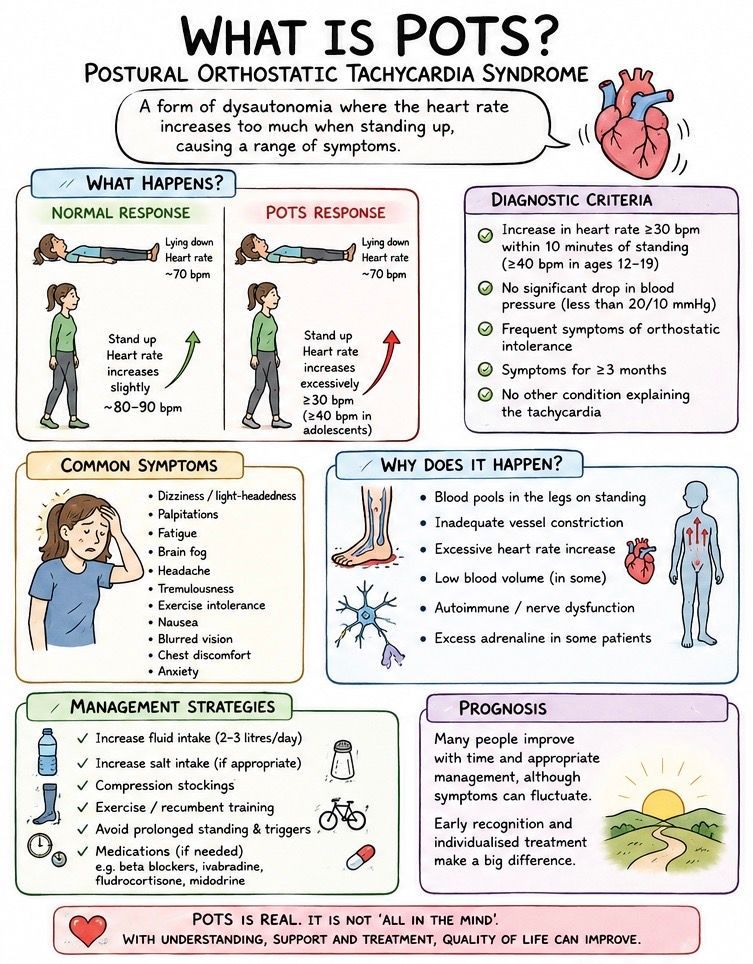
Postural Orthostatic Tachycardia Syndrome (POTS) is a complex and often misunderstood condition that affects the autonomic nervous system, causing an excessive increase in heart rate when moving from a lying or sitting position to standing. Although awareness of POTS has increased significantly in recent years, particularly following the COVID-19 pandemic, many patients still experience troublesome symptoms while waiting for an accurate diagnosis and appropriate treatment.
For some individuals, symptoms may be relatively mild and intermittent. For others, POTS can have a profound impact on quality of life, making everyday activities such as shopping, exercising, working, or even standing for prolonged periods extremely challenging. Many patients report years of unexplained symptoms before the underlying diagnosis is recognised.
POTS is not a heart disease in the traditional sense. The heart itself is usually structurally normal. Instead, the condition reflects a dysfunction of the autonomic nervous system—the body’s automatic control system responsible for regulating heart rate, blood pressure, breathing, digestion, temperature control, and many other vital functions.
As a consultant cardiologist, I frequently assess patients who present with symptoms such as palpitations, dizziness, light-headedness, fatigue, exercise intolerance, chest discomfort, and episodes of near-fainting. While these symptoms can arise from many different cardiac and non-cardiac conditions, POTS is increasingly recognised as an important cause, particularly among younger adults.
In this this article we explain what POTS is, why it develops, how it is diagnosed, and what treatment options are available. The aim is to provide an evidence-based overview that is accessible to patients while reflecting current scientific understanding.
What Does POTS Stand For?
POTS stands for Postural Orthostatic Tachycardia Syndrome.
Breaking down the term:
- Postural refers to changes in body position.
- Orthostatic means standing upright.
- Tachycardia means a faster-than-normal heart rate.
- Syndrome refers to a collection of symptoms and clinical findings that occur together.
The hallmark feature of POTS is an excessive rise in heart rate upon standing without a corresponding drop in blood pressure that would explain the symptoms.
The definition of POTS accepted by the Heart Rhythm Society in 2015 has three main components:
- An increase in heart rate of at least 30 beats per minute (bpm) within 10 minutes of standing in adults.
- An increase of 40 bpm or more in adolescents aged 12–19 years.
- Symptoms of orthostatic intolerance present for at least three months
- Absence of significant orthostatic hypotension.
- No alternative explanation for the tachycardia.
The definition of POTS accepted by the Heart Rhythm Society in 2015 has three main components. ¹
- POTS is a clinical syndrome characterized by symptoms that occur when standing upright. Common symptoms include: light-headedness, palpitations, shakiness, weakness, blurred vision, exercise intolerance and tiredness.
- Diagnostic criteria include a heart rate increase of ≥30 beats per minute (bpm) when moving from a lying (recumbent) position to standing for more than 30 seconds. In adolescents aged 12–19 years, the required heart rate increase is ≥40 bpm.
- There should be no orthostatic hypotension, meaning, no drop in systolic blood pressure of more than 20 mm Hg upon standing.
How Common is POTS?
Although once considered rare, POTS is increasingly recognised as a relatively common disorder.
Current estimates suggest that POTS affects approximately 0.2% to 1% of the population, although the true prevalence may be considerably higher due to underdiagnosis. Most patients present with POTS between 13 to 40 years, and according to different sources between 80 and over 90% are female.² ³ Many patients are otherwise healthy before symptom onset.
The condition appears particularly common in young women, although the reasons for this remain incompletely understood. Hormonal influences, autoimmune susceptibility, and differences in autonomic regulation may all play a role.
The COVID-19 pandemic has also led to a significant increase in recognised cases. Studies suggest that a proportion of patients with Long COVID develop symptoms and physiological abnormalities consistent with POTS, bringing greater attention to the condition among both clinicians and the public.14
Understanding the Autonomic Nervous System
To understand POTS, it is helpful to understand how the autonomic nervous system (ANS) normally works.
The autonomic nervous system operates largely without conscious control and regulates many essential bodily functions, including:
- Heart rate
- Blood pressure
- Breathing
- Digestion
- Body temperature
- Sweating
- Bladder function
- Blood vessel tone
The ANS has two main components:
The Sympathetic Nervous System
Often described as the “fight or flight” system, the sympathetic nervous system increases heart rate and blood pressure when the body needs to respond to stress or activity.
The Parasympathetic Nervous System
Often called the “rest and digest” system, the parasympathetic nervous system slows the heart rate and promotes recovery and relaxation.
A healthy autonomic nervous system continuously adjusts cardiovascular function to maintain adequate blood flow to the brain and other organs.
When we stand up, gravity causes approximately 700–900 mL of blood to shift into the legs and abdomen.⁶
Normally, specialised pressure sensors called baroreceptors detect this change and trigger compensatory responses:
- Blood vessels constrict.
- Heart rate increases slightly.
- Blood pressure remains stable.
- Blood flow to the brain is maintained.
In POTS, this finely tuned system does not function properly.
What Happens in POTS?
When a person with POTS stands up, blood tends to pool excessively in the lower body.
As a result:
- Less blood returns to the heart.
- Stroke volume falls.
- The body compensates by dramatically increasing heart rate.
- Cerebral blood flow may become impaired.
- Symptoms develop.
The increase in heart rate is often disproportionate to the physiological challenge.
A healthy person might experience a heart rate increase of 10–15 bpm when standing.
A patient with POTS may experience an increase of 30–60 bpm or more.
This excessive tachycardia can lead to symptoms such as:
- Palpitations
- Dizziness
- Light-headedness
- Fatigue
- Brain fog
- Tremulousness
- Exercise intolerance
Importantly, blood pressure is usually maintained, distinguishing POTS from classic orthostatic hypotension.¹
Why Does POTS Occur?
POTS is now recognised as a heterogeneous condition rather than a single disease.
Different patients may develop POTS through different mechanisms, as described below.
1. Neuropathic POTS
Some patients have partial autonomic neuropathy affecting the nerves responsible for constricting blood vessels in the legs.
As a result:
- Blood vessels fail to constrict adequately.
- Blood pools in the lower limbs.
- The heart compensates with rapid acceleration in heart beat.
2. Hyperadrenergic POTS
Other patients exhibit excessive activation of the sympathetic nervous system.
Features may include:
- Elevated plasma norepinephrine levels
- Palpitations
- Tremor
- Anxiety-like symptoms
3. Hypovolaemic POTS
Some patients appear to have lower-than-normal circulating blood volume.
Reduced blood volume means that standing produces a larger physiological challenge, triggering a more dramatic heart rate response.
Autoimmune Mechanisms and POTS
In recent years, increasing evidence has suggested that autoimmunity may play an important role in some patients with POTS.
An autoimmune condition occurs when the body’s immune system (antibodies) mistakenly attacks its own tissues. Although the precise significance of these antibodies remains an area of ongoing research, they may help explain why some patients develop POTS following:
- Viral infections
- Pregnancy
- Surgery
- Major physiological stress
- Vaccination
- Autoimmune disease
Patients with POTS are also more likely to have associated autoimmune disorders such as:
- Hashimoto’s thyroiditis
- Coeliac disease
- Sjögren’s syndrome
- Rheumatoid arthritis
- Systemic lupus erythematosus
This association does not necessarily mean that autoimmunity causes all cases of POTS, but it strongly suggests that immune dysregulation contributes to disease development in at least a subset of patients.
Long COVID and POTS
One of the most important developments in autonomic medicine over the past few years has been the recognition of POTS following COVID-19 infection.
Since the pandemic, clinicians worldwide have reported large numbers of patients presenting with:
- Persistent palpitations
- Fatigue
- Dizziness
- Exercise intolerance
- Brain fog
- Orthostatic symptoms
Many of these patients fulfil diagnostic criteria for POTS.
Several studies have suggested that autonomic dysfunction may represent one of the major mechanisms underlying Long COVID symptoms.14
Although the exact mechanisms remain uncertain, proposed explanations include:
Persistent Inflammation
COVID-19 may trigger prolonged inflammatory responses that affect autonomic regulation.
Autoimmune Activation
The infection may stimulate production of autoantibodies that interfere with cardiovascular control.
Small Fibre Neuropathy
Some patients demonstrate evidence of damage to small autonomic nerve fibres following infection.
Deconditioning
Periods of prolonged illness and reduced activity can contribute to cardiovascular deconditioning, which may exacerbate orthostatic symptoms.
What Are the Symptoms of POTS?
The symptoms of POTS can vary considerably between individuals.
Some patients experience mild intermittent symptoms, while others experience disabling daily symptoms affecting education, employment, and social activities.
Common symptoms include:
Cardiovascular Symptoms
- Palpitations
- Rapid heartbeat
- Awareness of heartbeat
- Chest discomfort
- Breathlessness
- Exercise intolerance
Many patients report feeling as though their heart is “racing” after standing up, walking upstairs, or performing relatively minor physical activities.
Although these symptoms can be alarming, the heart is usually structurally normal.
Neurological Symptoms
Neurological symptoms are among the most troublesome aspects of POTS.
These include:
- Dizziness
- Light-headedness
- Near-fainting
- Headaches
- Visual disturbances
- Difficulty concentrating
Patients frequently describe a sensation that they might faint when standing still.
Interestingly, complete loss of consciousness is less common than presyncope (near-fainting).
Brain Fog
“Brain fog” is one of the most frequently reported symptoms.
Although not a formal medical diagnosis, brain fog refers to difficulties with:
- Concentration
- Attention
- Memory
- Mental processing speed
- Word finding
Many patients report feeling mentally exhausted despite appearing physically well.
This symptom can have a profound impact on education, employment, and quality of life
Fatigue
Fatigue is often the dominant symptom in POTS.
Unlike normal tiredness, patients frequently describe:
- Severe exhaustion
- Lack of energy
- Delayed recovery after activity
- Reduced exercise capacity
- Many patients find fatigue more disabling than the tachycardia itself.
Gastrointestinal Symptoms
The autonomic nervous system plays an important role in digestive function.
Consequently, gastrointestinal symptoms are common and may include: nausea, bloating, abdominal pain, constipation and diarrhoea
Temperature Regulation and Sweating
Patients may also experience: heat intolerance, excessive or reduced sweating, flushing or difficulty in regulating body temperature. Warm environments frequently worsen symptoms because heat causes blood vessels to dilate, increasing blood pooling in the legs.
How is POTS Diagnosed?
Diagnosing POTS requires a careful clinical assessment. Unfortunately, many symptoms overlap with other conditions, meaning diagnosis may be delayed.
The diagnostic process generally includes:
Detailed Medical History
A careful history remains the most important diagnostic tool.
Questions typically focus on:
- Symptom triggers
- Positional symptoms
- Duration of symptoms
- Exercise tolerance
- Associated illnesses
- Medication use
- Family history
Patients often report symptoms that worsen on:
- Standing
- Hot days
- After meals
- During illness
- Around menstruation
Physical Examination
Clinical examination should include:
- Heart rate
- Blood pressure
- Orthostatic vital signs
- Cardiovascular examination
- Neurological assessment
In many patients the examination is otherwise normal.
A simple and useful bedside test which involves:
- Resting supine for at least 5 minutes.
- Recording heart rate and blood pressure, with diagnosis made if a difference of 30 beats per minute is observed.
- Standing upright.
- Repeating measurements over 5-10 minutes.
Patients with POTS typically demonstrate:
- Significant increase in heart rate
- Minimal blood pressure reduction
- Reproduction of symptoms
This simple test can often provide valuable diagnostic information.
Tilt-Table Testing
During the test:
- The patient is secured to a motorised table.
- Continuous heart rate and blood pressure monitoring is performed.
- The table is tilted upright, usually to 60–70 degrees.
The test reproduces the physiological effects of standing while allowing controlled monitoring.
Findings consistent with POTS include:
- Heart rate increase ≥30 bpm
- Orthostatic symptoms
- Absence of significant hypotension
Heart Investigations
Because symptoms such as palpitations and chest discomfort may suggest underlying cardiac disease, cardiology investigations are frequently performed.
These may include: electrocardiogram (ECG), echocardiography, ambulatory ECG monitoring (Holter) and exercise testing.
How is POTS Treated?
Although there is currently no universal cure for POTS, many patients experience substantial improvement with a combination of lifestyle measures, physical rehabilitation and, where appropriate, medication.
Treatment should always be individualised because POTS is a heterogeneous condition with several underlying mechanisms.
Most modern treatment strategies focus on:
- Improving blood volume
- Reducing blood pooling
- Optimising autonomic function
- Improving exercise tolerance
- Controlling symptoms
- Enhancing quality of life
The Heart Rhythm Society and Canadian Cardiovascular Society both emphasise that non-pharmacological measures should form the foundation of management.¹ ²
Increasing Fluid Intake
One of the simplest and most effective interventions is increasing daily fluid intake.
Patients with POTS are commonly advised to consume approximately:
2–3 litres of fluid daily
Adequate hydration helps:
- Increase circulating blood volume
- Improve venous return
- Reduce orthostatic symptoms
- Minimise tachycardia
Many patients notice symptom worsening during periods of dehydration, illness, hot weather, or prolonged travel.
Water remains the most important fluid, although electrolyte-containing drinks may also be helpful in selected patients.
Increasing Salt Intake
Provided there are no contraindications such as severe hypertension, heart failure or significant kidney disease, increased sodium intake is often recommended.
Typical targets range between:
8–10 grams of salt per day
This strategy helps expand plasma volume and improve blood pressure regulation.³
Compression Stockings
Compression stockings and other garments help reduce blood pooling in the legs and abdomen.
Evidence suggests that garments extending to the waist are generally more effective than knee-length stockings.
Useful options include:
- Compression tights
- Abdominal binders
- Full-length compression garments
Studies demonstrate improvements in orthostatic tolerance and symptom control in many patients.⁴
Exercise Rehabilitation: One of the Most Effective Treatments
Exercise training is now considered one of the most effective long-term treatments for POTS.
Historically, patients were often advised to avoid exertion because exercise triggered symptoms. However, research has shown that carefully structured exercise programmes can significantly improve cardiovascular function and quality of life.⁵ The key principle is gradual progression. Patients usually begin with: recumbent exercise (recumbent cycling, rowing machines or swimming). These activities minimise the effects of gravity while improving cardiovascular fitness. As symptoms improve, patients may gradually transition to upright cycling, walking or resistance training
Several studies have demonstrated significant reductions in tachycardia and improvements in symptoms following supervised exercise programmes.⁶
Avoiding Symptom Triggers
Patients often learn to recognise factors that exacerbate symptoms and avoidance strategies can substantially reduce symptom burden.
Common triggers include:
- Dehydration
- Hot weather
- Hot baths or showers
- Prolonged standing
- Alcohol
- Sleep deprivation
- Large meals
- Acute illness
Medications Used in POTS
Medication is usually considered when lifestyle measures alone are insufficient.
No drug is currently licensed specifically for POTS in the United Kingdom, but several medications are commonly used based on clinical evidence and specialist experience.
Beta-Blockers
Low-dose beta-blockers can reduce excessive heart rate responses.
Examples include:
- Propranolol
- Bisoprolol
- Metoprolol
Studies suggest that low-dose propranolol may improve symptoms while avoiding excessive fatigue that can occur with higher doses.⁷
Potential side effects include: fatigue, lower blood pressure, dizziness and reduced exercise tolerance
Ivabradine
Ivabradine slows heart rate by inhibiting the sinus node without affecting blood pressure.
Several studies have shown improvements in:
- Palpitations
- Orthostatic symptoms
- Quality of life
Because ivabradine does not typically lower blood pressure, it is often particularly useful in patients with low baseline blood pressure.⁸ Especially in patients with hyperadrenergic POTS as the predominant subtype
In our practice, ivabradine has become an increasingly popular option for selected patients with symptomatic POTS.
Midodrine
Midodrine increases blood vessel constriction and helps counteract excessive venous pooling.
Benefits may include:
- Improved standing tolerance
- Reduced dizziness
- Reduced tachycardia
Midodrine is particularly helpful when low blood pressure contributes to symptoms.⁹
Potential side effects include: tingling sensations and elevated blood pressure when lying down
Fludrocortisone
Fludrocortisone promotes sodium and water retention, increasing blood volume.
Potential benefits include:
- Improved blood pressure regulation
- Improved orthostatic tolerance
However, monitoring may be required because side effects can include: fluid retention, low potassium levels and elevated blood pressure
Pyridostigmine
Pyridostigmine enhances autonomic nervous system signalling and may reduce tachycardia in some patients.
Evidence suggests modest benefits in selected individuals, particularly when autonomic dysfunction is prominent.¹⁰
Can POTS Be Cured?
This is one of the most common questions patients ask and the answer is complex.
Some patients experience complete resolution of symptoms, particularly younger individuals and those whose symptoms develop following a temporary trigger such as infection.
Others experience:
- Gradual improvement
- Stable symptoms
- Relapsing-remitting symptoms
A smaller proportion continue to experience significant symptoms long term.
Current evidence suggests that while POTS may not always be curable, meaningful improvement is achievable for many patients through comprehensive management.¹¹
What is the Long-Term Prognosis?
Fortunately, POTS is not generally associated with increased mortality.
The condition can be highly debilitating, but it is not usually life-threatening.
Long-term studies suggest:
- Many adolescents improve significantly over time.
- Many adults experience gradual symptom improvement.
- Functional status often improves with treatment.
- Quality of life can be substantially enhanced through multidisciplinary management.
Nevertheless, symptoms may persist for years in some individuals. Early diagnosis and evidence-based treatment appear to improve outcomes.11
Frequently Asked Questions
Is POTS a Heart Condition?
Not primarily. POTS is usually considered a disorder of autonomic regulation rather than structural heart disease. Most patients have a normal heart on echocardiography.
Can POTS Cause Heart Damage?
Current evidence suggests that POTS itself does not damage the heart. The elevated heart rate reflects autonomic dysfunction rather than a pathological process affecting the heart muscle.
Can Anxiety Cause POTS?
Anxiety and POTS can coexist, but research clearly demonstrates that POTS is a genuine physiological disorder and should not be dismissed as anxiety alone.¹³
Can You Exercise With POTS?
Yes. Exercise is one of the most important treatments, although programmes should be introduced gradually and often benefit from specialist guidance.
Is POTS Related to Long COVID?
Yes. Growing evidence indicates that autonomic dysfunction, including POTS, contributes to symptoms experienced by some patients with Long COVID.¹⁴
Key Take-Home Messages
- POTS is a disorder of autonomic nervous system regulation.
- It causes an excessive increase in heart rate upon standing.
- Symptoms include palpitations, dizziness, fatigue, brain fog and exercise intolerance.
- The condition predominantly affects young women but can occur in anyone.
- Long COVID has increased awareness of POTS worldwide.
- Diagnosis is based on characteristic symptoms and objective heart rate changes during standing.
- Treatment focuses on hydration, salt intake, exercise rehabilitation and selected medications.
- The condition is not usually life-threatening.
- Many patients experience meaningful improvement with appropriate management.
References and further reading below
- Sheldon RS, Grubb BP, Olshansky B, et al. 2015 Heart Rhythm Society Expert Consensus Statement on the Diagnosis and Treatment of POTS, Inappropriate Sinus Tachycardia and Vasovagal Syncope. Heart Rhythm. 2015;12(6):e41-e63.
- Raj SR, Guzman JC, Harvey P, et al. Canadian Cardiovascular Society Position Statement on POTS and Related Disorders. Can J Cardiol. 2020.
- Raj SR. Postural Tachycardia Syndrome (POTS). Circulation. 2013;127:2336-2342.
- Bourne KM, Chew DS, Stiles LE, et al. Compression Garment Treatment in Orthostatic Intolerance. JACC. 2021.
- Fu Q, Vangundy TB, Shibata S, et al. Exercise Training versus Propranolol in POTS. Hypertension. 2011;58:167-175.
- Fu Q, Levine BD. Exercise and Non-Pharmacological Treatment of POTS. Autonomic Neuroscience. 2018.
- Raj SR, Black BK, Biaggioni I, et al. Propranolol Decreases Tachycardia and Improves Symptoms in POTS. Circulation. 2009.
- Taub PR, Zadourian A, Lo HC, et al. Randomized Trial of Ivabradine in POTS. J Am Coll Cardiol. 2021.
- Garland EM, Celedonio JE, Raj SR. Pharmacotherapy for POTS. Autonomic Neuroscience. 2015.
- Kanjwal K, Karabin B, Sheikh M, et al. Pyridostigmine in POTS. Pacing Clin Electrophysiol. 2011.
- Arnold AC, Ng J, Raj SR. Postural Tachycardia Syndrome – Diagnosis, Physiology and Prognosis. Autonomic Neuroscience. 2018.
- Boris JR, Bernadzikowski T. Long-Term Outcomes in Adolescents with POTS. Pediatric Cardiology. 2018.
- Bryarly M, Phillips LT, Fu Q, Vernino S, Levine BD. Postural Orthostatic Tachycardia Syndrome: JACC Focus Seminar. J Am Coll Cardiol. 2019;73(10):1207-1228.
- Narasimhan B, Hohler AD. Post-COVID-19 POTS Review. Frontiers in Neurology. 2023.
- Vernino S, Bourne KM, Stiles LE, et al. Postural Orthostatic Tachycardia Syndrome (POTS): State of the Science Review. Canadian Journal of Cardiology. 2021.
- Fedorowski A. Postural Orthostatic Tachycardia Syndrome: Clinical Presentation and Management. Journal of Internal Medicine. 2019.
- Benarroch EE. Postural Tachycardia Syndrome: A Heterogeneous and Multifactorial Disorder. Mayo Clinic Proceedings. 2012.
- Vernino S, Stiles LE. Autoimmunity in POTS. Autonomic Neuroscience. 2018.
- Wells R, Spurrier AJ, Linz D, et al. Postural Tachycardia Syndrome: Current Perspectives. Vascular Health and Risk Management. 2018.
- Steinberg RS, Sheldon RS. Contemporary Review of POTS. Progress in Cardiovascular Diseases. 2023.
About the Author
Dr Bart Olechowski MD MRCP(UK) DM is a Consultant Interventional Cardiologist practising in Hampshire, United Kingdom. He specialises in the assessment and management of cardiovascular conditions including palpitations, syncope, arrhythmias, coronary artery disease, and autonomic disorders. He consults through www.drbart.co.uk and www.winchesterandbasingstokecardiology.co.uk .
The above article was written with the assistance of AI and checked by the author for the accuracy.